医脉通APP

医脉通微信
公众号
问题反馈
医脉通APP
医脉通微信
公众号
问题反馈
说明:第53届美国血液年会的会议报告摘要已经发了4期了,看了一下,大家好像不是很感兴趣,因此就不再发啦~后面还有白血病、淋巴瘤、骨髓移植等内容的报告摘要,如果大家想看哪方面再联系我吧~~
主题: Myelodysplastic Syndromes: Results of Clinical Trials in Patients with MDS
时间:2011-12-11
标题:
2楼:A Decision Analysis of Reduced-Intensity Conditioning Allogeneic Hematopoietic Stem Cell Transplantation for Older Patients with De-Novo Myelodysplastic Syndrome (MDS): Early Transplantation Offers Survival Benefit in Higher-Risk MDS
3楼:Decision Analysis of Allogeneic Stem Cell Transplantation in Patients with Myelodysplastic Syndrome Stratified According to the Who Classification-Based Prognostic Scoring System (WPSS)
4楼:Treatment with the Thrombopoietin (TPO)-Receptor Agonist Romiplostim in Thrombocytopenic Patients (Pts) with Low or Intermediate-1 (Int-1) Risk Myelodysplastic Syndrome (MDS): Results of a Randomized, Double-Blind, Placebo(PBO)-Controlled Study
5楼:Phase 1 Dose-Escalation/Expansion Study of the p38/Tie2 Inhibitor ARRY-614 in Patients with IPSS Low/Int-1 Risk Myelodysplastic Syndromes
6楼:Lenalidomide Treatment Is Not Related to AML Progression Risk but Is Associated with a Survival Benefit in RBC Transfusion-Dependent Patients with IPSS Low- or Int-1-Risk MDS with del5q: Results From a Comparative Study
7楼:Radiation Treatment for Localized Prostate Cancer and the Risk of Developing Myelodysplastic Syndromes (MDS)
题目:A Decision Analysis of Reduced-Intensity Conditioning Allogeneic Hematopoietic Stem Cell Transplantation for Older Patients with De-Novo Myelodysplastic Syndrome (MDS): Early Transplantation Offers Survival Benefit in Higher-Risk MDS
作者:
John Koreth, MBBS, DPhil1, Joseph Pidala, MD, MS2, Waleska S. Perez, MPH3*, H. Joachim Deeg, M.D.4, Guillermo Garcia-Manero5, Luca Malcovati6*, Mario Cazzola6, Sophie Park7*, Raphael Itzykson, MD8*, Lionel Ades9,10, Pierre Fenaux, MD, PhD11, Martin Jädersten, MD, PhD12*, Eva Hellstrom-Lindberg, MD, PhD13, Robert Peter Gale, MD, PhD, DSc14, C. L. Beach, PharmD15*, Peter L. Greenberg, MD16, Martin S. Tallman, MD17, John F. DiPersio, MD, PhD18, Donald Bunjes, MD19*, Daniel J. Weisdorf, MD20 and Corey S. Cutler, MD, MPH, FRCPC1
1Division of Hematologic Malignancies, Dana-Farber Cancer Institute, Boston, MA
2Blood and Marrow Transplantation, Moffitt Cancer Center, Tampa, FL
3Medical College of Wisconsin, Milwaukee, WI
4Fred Hutchinson Cancer Research Center, Seattle, WA
5Leukemia, MD Anderson Cancer Center, Houston, TX
6Dept of Hematology Oncology, Fondazione IRCCS Policlinico San Matteo & University of Pavia, Pavia, Italy
7Hematology, Hôpital Cochin, Université Paris V, Paris, France
8Service d'Hematologie, Hopital Avicenne, Bobigny, France
9Groupe Francophone des Myelodysplasies, Bobigny, France
10Hematology Department, Avicenne Hospital APHP University Paris XIII, Bobigny, France
11Hôpital Avicenne, AP-HP, Université Paris 13, Bobigny, France
12Karolinska Institutet, Department of Medicine, Division of Hematology, Stockholm, Sweden
13Dept. of Med., Div. of Hem., Karolinska Institutet, Stockholm, Sweden
14Celgene Corp., Summit, NJ
15Celgene Corp, Summit, NJ
16Stanford Cancer Center Hematology Division, Stanford University, Stanford, CA
17Leukemia Service, Memorial Sloan-Kettering Cancer Center, New York, NY
18Department of Medicine, Division of Oncology, Washington University School of Medicine, St. Louis, MO
19Internal Medicine III, University of Ulm, Ulm, Germany
20Blood and Marrow Transplant Program, University Of Minnesota Medical Center, Minneapolis, MN
摘要:
Reduced-intensity conditioning (RIC) allogeneic hematopoietic stem cell transplantation is a curative approach for older patients with myelodysplastic syndrome (MDS), but is associated with early mortality risk. We previously used decision modeling to define the role of myeloablative transplantation in younger MDS patients aged <60 years, stratified by IPSS risk (Cutler et al, Blood 2004). We thereafter undertook a similar analysis to define the role of RIC transplantation in older MDS patients.
We constructed a Markov decision model in de-novo MDS patients aged 60-70 years to evaluate life expectancy after a strategy of early T-replete RIC transplantation versus standard-of-care non-transplantation approaches. Patients with chronic myelomonocytic leukemia, isolated 5q-, unclassifiable and therapy-related MDS were excluded. Patients undergoing transplantation with anti-thymocyte globulin or alemtuzumab-based conditioning or HLA mismatched or umbilical cord donors were also excluded. We undertook adjustments for quality-of-life (QoL) using standard utility estimates for different MDS and transplantation states (0.84: RBC transfusion-independent low/intermediate-1 MDS; 0.6: RBC transfusion-dependent low/intermediate-1 MDS; 0.53: intermediate-2/high MDS; 0.92: post transplantation-overall; 0.6: post transplantation-GVHD)
We evaluated survival of 92 patients after HLA matched RIC transplantation (Dana-Farber, Fred Hutchinson and CIBMTR datasets) stratified by IPSS risk state, versus survival with: best supportive care for 183 non-anemic low/intermediate-1 IPSS patients (IMRAW and Pavia datasets); hematopoietic growth factors for 78 anemic low/intermediate-1 IPSS patients (Nordic MDS Group and GFM datasets); and hypomethylating agents for 160 intermediate-2/high IPSS risk patients (Celgene AZA-001, GFM compassionate use azacytidine and M. D. Anderson decitabine datasets).
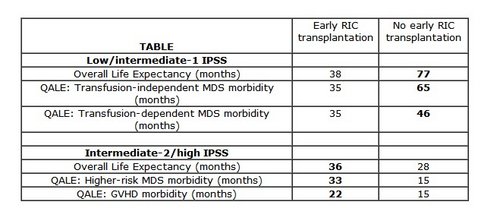
For older patients with low/intermediate-1 IPSS risk, early RIC transplantation impaired life expectancy compared to non-transplantation approaches (Table). Excluding patients transplanted beyond 12 months from diagnosis did not alter the conclusion. QoL adjustment narrowed the gap in quality adjusted life expectancy (QALE), but sensitivity analysis did not support RIC transplantation as the preferred strategy across a broad range of possible utility estimates (0.5-1), indicating that MDS-associated morbidity (e.g. RBC transfusion-dependence) does not favor early transplantation unless its QoL impact is substantial (state utility <0.4).
For older patients with intermediate-2/high IPSS risk, early RIC transplantation improved life expectancy compared with hypomethylating agents (Table). Excluding patients transplanted beyond 12 months from diagnosis did not alter the conclusion. However, transplantation is associated with early mortality such that the life expectancy benefit was apparent only after modeling survival beyond 5 years. Importantly, QoL adjusted survival benefit of transplantation was apparent both at 5 years and beyond, highlighting the morbidity of higher-risk MDS. In sensitivity analyses, QoL adjustment across the range of plausible transplantation-associated utility estimates (0.5-1) did not change the conclusion of QALE benefit.
We conclude that for de-novo MDS patients aged 60-70 years with low/intermediate-1 disease, early transplantation is not the preferred strategy unless MDS-associated QoL impairment is substantial. For intermediate-2/high IPSS risk, early RIC transplantation offers a life expectancy benefit, with quality adjusted survival benefit detectable earlier.
题目: Decision Analysis of Allogeneic Stem Cell Transplantation in Patients with Myelodysplastic Syndrome Stratified According to the Who Classification-Based Prognostic Scoring System (WPSS)
作者:Emilio Paolo Alessandrino1*, Matteo G Della Porta1*, Luca Malcovati1*, Christopher H Jackson2*, Cristiana Pascutto1*, Andrea Bacigalupo3, Maria Teresa van Lint3*, Michele Falda4*, Massimo Bernardi5*, Francesco Onida6, Stefano Guidi7*, Anna Paola Iori8*, Raffaella Cerretti9*, Paola Marenco10*, Pietro Pioltelli11*, Emanuele Angelucci12, Rosi Oneto3*, Alessandro Rambaldi13, Alberto Bosi7 and Mario Cazzola1 1Dept of Hematology Oncology, Fondazione IRCCS Policlinico San Matteo & University of Pavia, Pavia, Italy 2MRC Biostatistics Unit, Institute of Public Health, Cambridge, United Kingdom 3Dept of Hematology Oncology, Ospedale San Martino, Genova, Italy 4Stem Cell Transplant Center,, Ospedale San Giovanni Battista, Torino, Italy 5Hematology and Bone Marrow Transplantation Unit, IRCCS Ospedale San Raffaele, Milano, Italy 6Division of Hematology, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, University of Milan, Milano, Italy 7Dept of Hematology, Ospedale di Careggi, Firenze, Italy 8Dept of Cellular Biotechnologies and Hematology, Sapienza University of Rome, Roma, Italy 9Stem Cell Transplant Unit, University of Rome Tor Vergata, Roma, Italy 10Dept of Hematology Oncology, Ospedale Niguarda Ca' Granda, Milano, Italy 11Div of Hematology and Transplant Unit,, Ospedale San Gerardo, Monza, Italy 12Hematology and Bone Marrow Transplantation Unit, Ospedale Oncologico Armando Businco, Cagliari, Italy 13Div of Hematology, Ospedali Riuniti, Bergamo, Italy
摘要: Myelodysplastic syndromes (MDS) are heterogeneous myeloid neoplasms that range from indolent conditions with a near normal life expectancy to forms very close to acute myeloid leukemia (AML). The WHO classification-based Prognostic Scoring System (WPSS) is able to classify MDS patients into five risk groups (very low, low, intermediate, high, and very high) with different median survival (from more than 10 to about 1 yr). Despite recent progress, the only curative treatment for MDS remains allogeneic stem cell transplantation (allo-SCT), which however involves a non-negligible risk of mortality and morbidity. Allo-SCT is not considered in patients with low WPSS risk, whose median survival is >10 yr. Conversely, eligible patients with high or very high WPSS risk, whose median survival is 1-2 yr, should be offered immediate transplantation. Uncertainty exists about the optimal timing of allo-SCT in the low and intermediate WPSS-risk groups, and to address this issue we performed an ad hoc decision analysis. We analyzed two cohorts of MDS patients: i) 615 patients diagnosed with MDS at the Fondazione IRCCS Policlinico San Matteo, Pavia, Italy, between 1992-2007, who were followed regularly and mostly received best supportive care; ii) 405 patients who received allo-SCT between 1997-2007, reported to the Gruppo Italiano Trapianto di Midollo Osseo (GITMO) registry. In this latter cohort, variables were analyzed at the time of transplantation in patients undergoing allo-SCT upfront, and at the time of remission-induction chemotherapy in those receiving treatment before allo-SCT. We adopted a continuous time multi-state Markov approach to model the natural history of the disease. In this model, each WPSS risk group is represented by a state, and transition is allowed to the next state (to AML from very high risk) or to death. A transition intensity (i.e., instantaneous risk of moving to another state) is then estimated for each possible transition. Allo-SCT is modeled as a time-dependent covariate with 3 levels: i) no allo-SCT; ii) transplantation done no more than 3 months before; iii) transplantation done more than 3 months before. The effect of allo-SCT on survival was estimated by hazard ratios (HR) with respect to the no allo-SCT level. We examined two different policies: policy A) to perform allo-SCT after t months since entering the low-risk state or at the time of progression to intermediate risk; policy B) to perform allo-SCT after t months since entering the intermediate-risk state or at the time of progression to high risk. For each policy, the expected survival of patients with different age at diagnosis was calculated. According to the model, a patient with a low WPSS risk is expected to spend 6.2 years (95% CI, 5.5-7.0) in this risk group, and, in case of progression, 3.5 years (95% CI, 3.1-4.0) in the intermediate one. The cumulative incidence of progression from low to a higher WPSS risk was 9%, 31% and 41% at 1, 3 and 5 years, respectively, while that of progression from intermediate to a higher risk was 18%, 40% and 53% at 1, 3 and 5 years, respectively. Overall, expected survival times from diagnosis were higher under policy A vs policy B. Expected survival decreased with increasing age (from 30 to 65 yr) under policy A, while there was little effect of age under policy B. For younger patients, expected survival times were up to four years greater under policy A, while there was no estimated benefit for patients closer to age 65. When the waiting time before transplantation was progressively increased from 0 to 60 months, there was a small decrease in expected survival under policy A for younger patients. Conversely, varying the time of transplantation between 0-60 months did not substantially influence expected survival under policy B. These findings suggest that in eligible patients with low or intermediate WPSS-risk MDS there is no clear benefit in adopting a delayed transplantation strategy, as the risk of progression abolishes the expected gain in survival resulting from postponing the procedure. In particular, younger patients appear to benefit from early transplantation in the low risk state. This is at variance with a previous decision analysis based on the International Prognostic Scoring System (IPSS) (Blood. 2004;104:579-85), which concluded that for low and intermediate-1 IPSS-risk MDS, delayed allo-SCT was associated with maximal life expectancy. This paper is on behalf of GITMO investigators.
题目: Treatment with the Thrombopoietin (TPO)-Receptor Agonist Romiplostim in Thrombocytopenic Patients (Pts) with Low or Intermediate-1 (Int-1) Risk Myelodysplastic Syndrome (MDS): Results of a Randomized, Double-Blind, Placebo(PBO)-Controlled Study
作者: Aristoteles Giagounidis, MD, PhD1, Ghulam J. Mufti, MD2, Hagop M. Kantarjian3, Pierre Fenaux, MD, PhD4, Mikkael A. Sekeres, MD, MS5, Jeffrey Szer, MBBS, FRACP6, Andrea Kuendgen, MD7*, Uwe Platzbecker, MD8, Gianluca Gaidano9*, Wieslaw Jedrzejczak10*, Kuolung Hu11*, Allen S. Yang, MD, PhD11 and Susie Jun11* 1St. Johannes Hospital, Duisburg, Germany 2Department of Haematological Medicine, King's College Hospital, London, United Kingdom 3Leukemia, MD Anderson Cancer Center, Houston, TX 4Hôpital Avicenne, AP-HP, Université Paris 13, Bobigny, France 5Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Cleveland, OH 6Clinical Haematology & BMT Service, The Royal Melbourne Hospital, Parkville, Victoria, Australia 7Heinrich-Heine University of Düsseldorf, Duesseldorf, Germany 8Medizinische Klinik und Poliklinik I, Universitätsklinikum Carl Gustav Carus, Dresden, Germany 9Department of Clinical and Experimental Medicine, Amedeo Avogadro University of Eastern Piedmont, Division of Hematology, Novara, Italy 10Medical Academy of Warsaw, Warsaw, Poland 11Amgen Inc., Thousand Oaks, CA
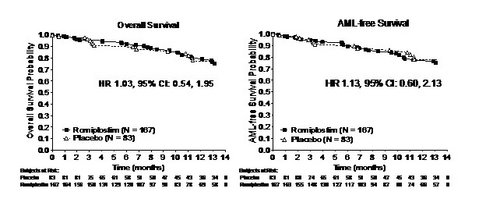
摘要: Background: There are few therapies for thrombocytopenia in MDS, which is found in ~50% of pts with low/int-1 MDS and is associated with shortened survival. Methods: IPSS low/int-1 MDS pts receiving supportive care, with platelets 1) ≤20x109/L or 2) ≤ 50x109/L with a history of bleeding, were randomized 2:1 to 750 µg romiplostim:PBO for 26 wk with MDS supportive care, and a 4-wk washout followed by bone marrow (BM) biopsy. Pts continued as randomized, with any MDS therapy, for 24 wk with another 4-wk washout followed by a BM biopsy. The 1° endpoint was the number of clinically significant bleeding events (CSBE, grade ≥2 per modified WHO scale); other endpoints included protocol-defined platelet transfusion events (PTE), platelet response per IWG 2006 (HI-P), survival, and safety, including progression to AML, defined conservatively as: 1) ≥20% blasts in the BM or peripheral blood after 4 wk off romiplostim, or 2) pathology consistent with leukemia (eg, chloroma or leukemia cutis), or 3) anti-leukemic treatment initiation. Results: Of 250 pts enrolled (romiplostim 167, PBO 83): 59% were male, median (Q1, Q3) age was 70 (61, 77) year, WHO classes RCMD (68%), RAEB-1 (13%), MDS-U (11%), RA (4.4%), RCMD-RS (2.4%), RARS (0.8%), RAEB-2 (1%), IPSS status low (25%), int-1 (71%), int-2 (0.4%), and IPSS cytogenetics good (78%), intermediate (18%), poor (1.6%). There were more pts who were RAEB-1 (14% vs 11%) and RAEB 2 (1% vs 0%) and fewer who were MDS-U (10% vs 15%) with romiplostim (all NS). Due to DMC concerns regarding the potential for transient increases in blast cell counts and the risk for progression to or treatment for AML, study drug was discontinued in Feb 2011, affecting 28% of pts. Also leading to withdrawal were consent withdrawn (romiplostim 13%, PBO 15%), adverse events (AE) (12%, 5%), and alternative therapy (7%, 11%). The mean number of CSBE/pt was romiplostim 1.47, PBO 1.94 (HR 0.83, 95% CI: 0.66, 1.05, p = 0.13); rates were romiplostim 18.6%, PBO 26.5%. The overall number of bleeding events was reduced with romiplostim (RR 0.92, 95% CI: 0.86, 0.99, p = 0.026). PTE rates/100 pt year were romiplostim 748.9, PBO 1013.5 (RR 0.77, 95% CI: 0.66, 0.88, p<0.001). HI-P rates were romiplostim 36.5% (61 pts), PBO 3.6% (3 pts) (OR 15.6, 95% CI: 4.7, 51.8, p<0.001). From wk 4 on, median platelets with romiplostim were consistently higher than with PBO (p<0.001). The overall 1-year K-M survival was romiplostim 80%, PBO 78% (HR 1.03, 95% CI: 0.54, 1.95) (Figure 1), with 28 deaths (17%), none (0%) hemorrhagic and 5 (3%) from AML and MDS disease progression, with romiplostim and 14 deaths (17%), including 4 (4.8%) hemorrhagic and 3 (3.6%) from AML and MDS disease progression, with PBO. Median time on romiplostim was 21.5 wk (range: 1, 50). SAE rates were romiplostim 40%, PBO 27%; those frequent (≥5%) SAE occurring ≥2x more with romiplostim were pneumonia, pyrexia, thrombocytopenia, and atrial fibrillation; those occurring ≥2x more with PBO were diarrhea, dyspnea, and cerebral hemorrhage. Peripheral blast increases are described below (Table).
AML rates through 58 wk were romiplostim 6.0%, PBO 2.4% (HR 2.51, 95% CI: 0.55, 11.47). Of the 13 AML cases, 9 (69%) were in pts who were initially RAEB-1 and 4 (31%) were diagnosed by anti-leukemic therapy initiation, which could include hypomethylating agents. Of pts who were RAEB-1 at baseline, 2/9 (22%) PBO pts developed AML vs 7/24 (29%) of romiplostim pts. AML-free survival rates were similar (HR 1.13, 95% CI: 0.60, 2.13). Conclusion: Romiplostim treatment in low/int-1 MDS pts resulted in a 15-fold increase in achieving HI-P. Although there were more platelet transfusions with PBO (p 10% occurred more frequently with romiplostim but generally resolved after romiplostim discontinuation. AML was defined conservatively; cases are pending central pathology review. AML occurred primarily in pts who were initially RAEB-1 and in more pts with romiplostim. Overall and AML-free survival rates were similar.
Disclosures: Giagounidis: Amgen: Consultancy; GlaxoSmithKline: Consultancy. Off Label Use: This trial examined the use of romiplostim, which is indicated for use in ITP, in MDS.. Mufti: Celgene: Consultancy, Research Funding. Kantarjian: Amgen: Research Funding. Fenaux: Celgene: Honoraria, Research Funding; Amgen: Honoraria; Roche: Research Funding; Janssen Cilag: Research Funding. Sekeres: Celgene Corp: Honoraria, Membership on an entity’s Board of Directors or advisory committees; Amgen: Membership on an entity’s Board of Directors or advisory committees. Kuendgen: Celgene: Honoraria. Platzbecker: Amgen: Honoraria; GSK: Honoraria. Gaidano: Amgen: Honoraria. Jedrzejczak: Amgen: Membership on an entity’s Board of Directors or advisory committees, Research Funding. Hu: Amgen: Employment, Equity Ownership.
题目:Phase 1 Dose-Escalation/Expansion Study of the p38/Tie2 Inhibitor ARRY-614 in Patients with IPSS Low/Int-1 Risk Myelodysplastic Syndromes
作者:
Rami S. Komrokji, MD1, Alan F. List, MD1, H. Jean Khoury, MD, FACP2, Jeffrey E. Lancet, MD1, Elias Jabbour, MD3, Maria C Foudray, RN3*, Shannon L Winski, PhD4*, Stacie Bell, PhD4*, Selena Armistead Rush, BS4*, Lara Maloney, BA4*, Ann Marie Ptaszynski, MD4*, Hagop M. Kantarjian3 and Guillermo Garcia-Manero5
1Malignant Hematology, H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL
2Winship Cancer Institute, Emory University School of Medicine, Atlanta, GA
3Department of Leukemia, University of Texas MD Anderson Cancer Center, Houston, TX
4Array BioPharma Inc., Boulder, CO
5Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX
摘要:
Background: Myelodysplastic syndromes (MDS) are characterized by excess elaboration of myelosuppressive cytokines contributing to increased apoptotic loss of hematopoietic precursors, the hallmark of lower-risk MDS. p38a MAP kinase (MAPK) is a key downstream convergence point and effector of hematopoietic inhibitory cytokines and death receptors in hematopoietic precursors and stromal elements. The actions of Tie2 complement this regulatory axis by promoting cytokine production and altering cellular quiescence. ARRY-614 is a small-molecule inhibitor of both p38 MAPK and Tie2 that may improve hematopoiesis in lower-risk MDS patients (pts).
Methods: This Phase 1 study was designed to determine the maximum tolerated dose (MTD) of ARRY-614 and evaluate safety, pharmacokinetics (PK), preliminary efficacy (International Working Group [IWG] 2006) and pharmacodynamic (PD) effects. Eligible pts had International Prognostic Scoring System (IPSS) risk group Low or Int-1 MDS, and had either received prior therapy or were not eligible or refused treatment. ARRY 614 was administered in 28 day cycles. A standard 3+3 dose escalation design was used and an expansion cohort at the MTD in red blood cell (RBC) transfusion-dependent (TD) pts was evaluated.
Results: Forty-five pts with Low (n = 11) or Int-1 (n = 34) risk MDS were enrolled with a median age of 72 years (range 47-84). All but one pt had disease refractory to and/or relapsed from prior therapy with a median of 3 prior regimens (range 0-10); 82% received hypomethylating agents (HMAs), 49% received erythropoietin (EPO) stimulating agents and 40% received lenalidomide. As of July 2011, 7 pts remain on study.
ARRY-614 was administered in a fasting state at doses of 400-1200 mg once daily (QD) and 200-300 mg twice daily (BID), and under fed conditions at 400 mg QD. Dose limiting toxicities (DLTs) reported at QD doses included single events of Grade (Gr) 3 diarrhea (400 mg QD fasting), Gr 3 macular skin rash (1200 mg QD) and Gr 3 QTc prolongation (400 mg QD fed). Due to the high number of capsules required per dose, the maximum administered QD dose was 1200 mg; the MTD was not reached. The 300 mg BID dose was dose limiting due to 5/7 pts with DLTs of Gr 3 rash (n = 2), Gr 3 asthenia and jitteriness (n = 1), Gr 3 allergic reaction to study medicine (n = 1), and Gr 3 muscle weakness with Gr 3 elevated AST/ALT (n = 1); therefore BID dosing was discontinued. The most common (≥ 10% of pts) treatment-related adverse events (AEs) across all dose cohorts included rash (29%), diarrhea (22%), dry skin (13%) and QTc prolongation (11%). The median duration of treatment was 16 wks (range 1 76).
ARRY-614 exposure was dose proportional, but high inter-pt variability was observed. The median Tmax was 3 hours and the t1/2 was ~ 8 hours; both parameters were consistent across all doses evaluated.
Plasma EPO was elevated at baseline in pts with erythroid response (471 ± 285 U/L, n = 4) and decreased by 92 ± 4% overall. In non-responding pts, baseline EPO was 984 ± 315 U/L (n = 41) and 68 ± 22% maximal decrease was observed. In 68% (13/19) of pts that were above 500 U/L at baseline, EPO was suppressed below 500 U/L during time on study supporting a drug effect in these pts as well.
Eight of 43 evaluable pts experienced hematological improvement (HI) per IWG 2006 criteria. HI responses (duration 8 to 80 wks) occurred in all lineages (4 HI-erythroid, 5 HI-neutrophil and 4 HI platelet) including 5 bi-lineage responses and some pts had a reduction in platelet transfusions. All IWG 2006 responders failed prior treatment with ≥ 1 HMA. At doses ≥ 900 mg QD, 6 of 18 evaluable pts achieved HI in one or more lineage.
Conclusions: ARRY-614 has shown encouraging preliminary multi lineage hematologic activity as a single agent in a heavily pretreated pt population. At the QD doses studied to date, it has demonstrated an acceptable safety profile. Correlative studies of preliminary drug activity with PD analyses from bone marrow samples are ongoing (final results to be presented). Given the variable but dose-proportional drug exposure, a new oral formulation with improved PK profile will be evaluated in MDS pts starting 4Q2011. Because ARRY-614 has promising preliminary activity, additional investigation in this lower-risk MDS population who have received prior treatment with HMAs is warranted. In addition, the treatment-related reductions in plasma EPO suggest that combination treatment with recombinant EPO may optimize erythroid response.
题目:Lenalidomide Treatment Is Not Related to AML Progression Risk but Is Associated with a Survival Benefit in RBC Transfusion-Dependent Patients with IPSS Low- or Int-1-Risk MDS with del5q: Results From a Comparative Study
作者:
Andrea Kuendgen, MD1*, Michael Lauseker2*, Alan F. List, MD3, Pierre Fenaux, MD, PhD4, Aristoteles Giagounidis, MD, PhD5, Nancy Brandenburg, PhD6*, Jay Backstrom, MD6, Axel Glasmacher, MD6, Joerg Hasford, MD2*, Ulrich Germing, MD1* and On behalf of the International Working Group on MDS with del5q1*
1Heinrich-Heine-Universität, Düsseldorf, Germany
2Ludwig-Maximilians Universität, Munich, Germany
3H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL
4Hôpital Avicenne, Bobigny, France
5St. Johannes Hospital, Duisburg, Germany
6Celgene Corporation, Summit, NJ
摘要:
Background: Lenalidomide (LEN) treatment resulted in RBC transfusion independence for ≥ 8 wks in 51–67% of patients (pts) and cytogenetic response in 25–73% of pts with lower-risk MDS and del5q in 2 large multicenter trials (MDS-003 and -004) (List A et al. NEJM 2006;355:1456-65; Fenaux P et al. Blood 2011; doi:10.1182/blood-2011-01-330126). However, these studies were either single-arm or allowed early crossover to LEN, thus data on the influence of LEN on AML progression and overall survival (OS) is lacking. Aims: To assess the risk of AML progression and death in LEN-treated MDS-003 and -004 pts vs untreated MDS pts with del5q from a large multicenter registry, and to determine relevant risk factors. Methods: Data from 459 MDS pts with del5q entered into local or regional MDS registries were retrospectively collected from 9 centers (Europe, USA, Australia) using a uniform minimal data set. Eligible pt controls had IPSS Low-/Int-1-risk MDS and were RBC transfusion-dependent (≥ 1 unit/8 wks), reflecting the relevant inclusion criteria for both trials, and received best supportive care only including ESAs. Incidence of AML progression was assessed using a cumulative incidence estimator in the presence of competing risk (ie, death), and considering left truncation (LT) for the LEN cohort. OS was assessed using a cumulative probability estimator considering LT. Cox proportional hazards (PH) models with LT were used to assess the impact of LEN treatment and baseline factors (ie, age, sex, cytogenetics, bone marrow [BM] blast %, transfusion burden, no. of cytopenias, hemoglobin [Hgb] level [g/dL], and platelet and neutrophil counts) on risk of AML progression and death. LT is a statistical method to correct for different starting points of follow-up (ie, date of first LEN dose in clinical trial pts vs date of diagnosis in registry pts). Results: We analyzed 295 LEN-treated and 125 untreated pts. Baseline characteristics of treated (at first LEN dose) vs untreated (at diagnosis) pts were similar: mean age 65.0 vs 66.2 yrs; female sex 71% vs 68%; IPSS Low-/Int-1-risk 43%/57% vs 43%/57%. Median observation time was 4.3 vs 4.6 yrs. Baseline RBC transfusion burden was higher in the LEN cohort (median [range] units/8 wks: 6 [1–25] vs 2 [1–10]). Two- and 5-yr cumulative AML incidences were 7% and 23% for LEN vs 12% and 20% for the untreated cohort. Two- and 5-yr cumulative OS probabilities were 90% and 54% for LEN vs 74% and 41% for the untreated cohort. Median time to AML progression has not been reached for either cohort. Median OS was 5.2 yrs (95% CI 4.5–5.9) for LEN-treated vs 3.8 yrs (95% CI 2.9–4.8) for untreated pts. In the final Cox PH models, LEN treatment (hazard ratio [HR] .939; p = .860) and 1 cytogenetic abnormality (abn) in addition to del5q (HR 1.111; p = .755) did not increase the risk of AML progression. Significant factors associated with an increased risk of AML progression were complex cytogenetics (del5q plus > 1 abn; HR 3.627; p = .002), BM blasts 5–10% (HR 2.215; p = .016), and higher transfusion burden (HR 1.097 [10% increase in risk per unit at baseline]; p = .029); higher Hgb levels were associated with a reduced risk (HR .857; p = .054). Regarding survival, LEN treatment was associated with a reduced risk of death (HR .597; p = .012). Other factors associated with decreased mortality were higher Hgb levels (HR .883; p = .028), higher platelet counts (HR .999; p = .035), and female sex (HR .598; p = .002). Higher transfusion burden (HR 1.056; p = .037) and age (HR 1.049; p < .001) increased the risk of death. In separate Cox PH models considering IPSS risk (Int-1 vs Low) and transfusion dependency for AML progression and OS, as well as age and sex for OS only, IPSS Int-1-risk was associated with an increased risk of AML progression (HR 1.689; p = .041) but not with an increased risk of death (HR 1.056; p = .723). Findings for LEN treatment when considering IPSS risk were similar to the final Cox PH models that considered individual covariates (AML progression: HR .892, p = .741; OS: HR .545; p = .003). Results were similar when Cox PH models were reanalyzed without LT. Conclusions: In this retrospective analysis of RBC transfusion-dependent pts with lower-risk MDS and del5q, LEN treatment was not associated with a higher risk of AML progression but led to a survival benefit vs untreated pts, despite a higher transfusion burden in the LEN cohort. Other significant risk factors for AML progression and death are consistent with previous findings in MDS pts.
题目:Radiation Treatment for Localized Prostate Cancer and the Risk of Developing Myelodysplastic Syndromes (MDS)
作者:Sudipto Mukherjee1*, Chandana Reddy2*, Jay Ciezki2*, Ramon V. Tiu, MD3, Edward A. Copelan, MD1, Anjali S. Advani, MD1, Yogen Saunthararajah, MD1, Katarina Paulic4*, Jaroslaw P. Maciejewski, MD, PhD1, Brian J. Bolwell5, Eric A. Klein, MD6* and Mikkael A. Sekeres, MD, MS1 1Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Cleveland, OH 2Radiation Oncology, Cleveland Clinic, Cleveland, OH 3Departments of Translational Hematology and Oncolgy Research and Hematologic Oncology and Blood Disorders, Cleveland Clinic, Cleveland, OH 4Hematologic Oncology and Blood Disorders, Cleveand Clinic Taussig Cancer Institute, Cleveland , OH 5Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Cleveland , OH 6Glickman Urological & Kidney Institute, Cleveland Clinic, Cleveland, OH
摘要:Background: Both environmental radiation exposure and use of therapeutic radiation (XRT) in primary solid tumor malignancies increase the risk of secondary MDS. No data exist on the risk of developing secondary MDS in prostate cancer patients (pts) being treated with radiotherapy. Establishing this risk has important clinical implications, as prostate cancer is the leading cancer in men and radiation therapy has increasingly become the preferred modality for treatment of localized prostate cancer. Methods: We performed a prospective case control study of 11,015 pts with localized prostate adenocarcinoma newly diagnosed between 1986 and 2011 at Cleveland Clinic who underwent treatment with either radical prostatectomy (control group) or definitive radiotherapy (external beam radiotherapy [EBRT] or prostate interstitial brachytherapy [PI] – case group), to investigate the risk of radiation-related MDS. Data on demographics, surgery, radiation treatment, and follow-up were collected from merged prostate cancer and MDS databases. Cytogenetic risk groups were per International Prognostic Scoring System (IPSS) for MDS. Univariate and multivariate analyses were performed using the Fine and Gray competing risk model with MDS as a time-dependent endpoint (which incorporates differences in duration of follow-up) and death from any cause as the competing event, comparing radiotherapy groups to the surgical cohort as the reference group, controlling for age and follow-up frequency. Hazard ratios (HR) with 95% confidence intervals (CIs) are reported. Results: For all pts, median age was 64 years (yrs, range, 37 – 88) at the time of prostate cancer diagnosis: 69 yrs in EBRT, 67 yrs in PI, and 60 yrs in surgery pts, respectively (p<0.0001); 5119 (46%) were treated with XRT, 5896 (54%) with prostatectomy. None of the pts had a previous history of another malignancy. Among XRT pts, 2183 (43%) were treated with EBRT, 2936 (57%) with PI. Median follow-up was 3.0 yrs [(range, 0.0 – 25.2): 6.8 yrs in the EBRT group, 2.5 yrs in the PI group and 1.8 yrs in the surgery group, (p<0.0001)] following prostate intervention, longer (4.6 yrs) in pts treated since 1996, when PI was first performed [6.6 yrs in the EBRT group, 3.8 yrs in the PI group and 4.3 yrs in the surgery group, (p<0.0001)]. In the entire cohort, 30 pts developed MDS: 24 in the XRT group and 6 in the surgery group. MDS World Health Organization classification was: RA/RARS (n=12), RCMD (n=3), RAEB-1 (n=3), RAEB-2 (n=3), CMML (n=2), MDS-U (n=3) and unknown (n=4). IPSS cytogenetic risk classification was: good risk (n=17), intermediate risk (n=5), poor risk (n= 4) and unknown (n = 4). For MDS pts within the XRT group, median age at MDS diagnosis was 79 yrs (range, 74 – 89) for EBRT, 80 yrs (range, 64 – 100) for PI. The median time to develop MDS was 8.9 yrs (range, 0.9 – 20.2): 9.1 for EBRT, 8.2 for PI, and 13.0 for prostatectomy pts, respectively (p=0.05). In univariate analyses, older pts (HR=1.14; CI, 1.09 – 1.2; p<0.0001), and those treated with XRT (HR=3.3; CI, 1.35 – 8.08; p=0.009): EBRT (HR=2.6; CI, 1.0 – 6.9; p=0.05), PI (HR=5.87; CI, 2.1 – 16.3; p=0.0007) were significantly more likely to develop MDS. In multivariate analysis though, while advanced age (HR=1.13; CI, 1.0 – 1.2; p < 0.0001) remained significantly associated with MDS development, XRT did not (HR=1.56; CI, 0.56 – 4.38; p=0.4), though a trend remained for PI (HR=2.85; CI, 0.9 – 8.8; p = 0.07). Conclusions: Pts who underwent definitive radiation treatment for localized prostate cancer did not appear to have a significantly increased risk of subsequent MDS, in analyses that controlled for age and incorporated length of follow-up. A trend for MDS development was present for those undergoing XRT with PI. These findings are encouraging for both patients and providers who have concerns about the potential effects of XRT on development of MDS.