尿道下裂TIP手术图解(Snodgrass technique for hypospadias repair)
资料来源:BJU international 2005。
文献作者:WARREN T. SNODGRASS。
文献题目:Snodgrass technique for hypospadias repair。
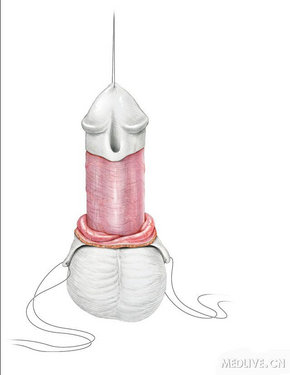
A 5–0 polypropylene suture is place into the glans for traction and to later secure the urethral stent. The initial skin incision depends upon whether the family prefers circumcision or foreskin reconstruction, as either can be performed. When circumcision is the desired result care is taken to preserve sufficient inner prepuce so that a so-called ‘mucosal collar’ can be approximated in the ventral midline after glansplasty. Then the penis is degloved to near the penoscrotal junction. If the foreskin is to be reconstructed the skin incision extends from the corners of the dorsal preputial hood to 2 mm proximal to the meatus. Ventral shaft skin is released until normal dartos tissues are encountered.
An artificial erection confirms the absence of ventral curvature, but if there is significant bending a midline dorsal plication is done using a single 6–0 polydioxanone suture placed in the tunica albuginea of the corpora cavernosa directly opposite the point of
maximum curvature.
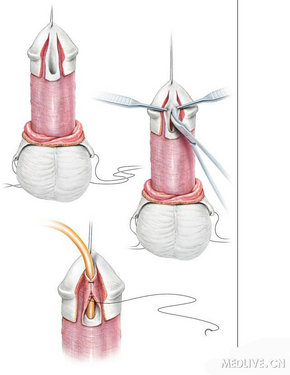
Figure 2
Next, longitudinal incisions are made along the visible junction of the glans wings to the urethral plate. Proposed lines for incision are first infiltrated with 1 : 100 000 noradrenaline or a tourniquet is used around the base of the penis for haemostasis. After making the skin incision with the 69 Beaver scalpel, I prefer to complete the dissection and glans wings mobilization using tenotomy scissors, taking care both to preserve vascularity to the urethral plate and sufficient thickness for the wings to be securely approximated.
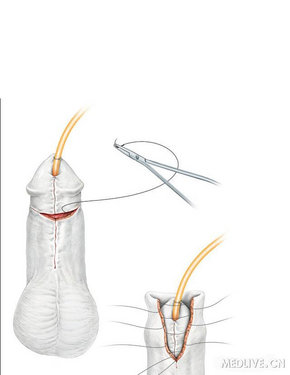
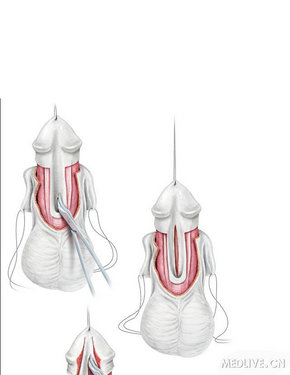
Figure 3
The key step in the procedure is midline incision of the urethral plate. This manoeuvre is facilitated by counter-traction maintained by the surgeon and assistant along opposite margins of the plate. Using tenotomy scissors, the relaxing incision is made from within the meatus to the tip of the urethral plate. It should not be carried further distally into the glans. The depth of incision depends upon whether the plate is grooved or relatively flat, but in all cases extends down to near the corpora cavernosa. Figure 3c: A 6 F Silastic stent is passed into the bladder and secured to the glans traction suture. Then the urethral plate is tubularized beginning at the neomeatus, using 7–0 polyglactin suture. The first suture is placed through the epithelium at a point just distal to the midglans so that the meatus has an oval, not rounded, configuration. Tubularization is completed with a running two-layer subepithelial closure, turning all epithelium into the neourethral lumen.
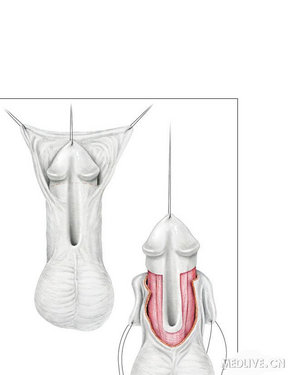
Figure 4
A dartos pedicle flap is dissected from thepreputial hood and dorsal shaft skin in patients undergoing circumcision, then button-holed and transposed ventrally to cover the entire neourethra. When the foreskin is reconstructed this layer is not accessible, yet there has been no increased incidence of fistula in my experience.
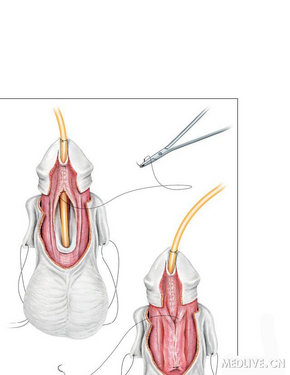
Figure 5
Glansplasty is a key determinant of the final cosmetic outcome. Over the years my technique has developed, and currently begins with a 7–0 polyglactin suture through the epithelium at the desired point for the ventral lip of the meatus. A second 7–0 suture is placed subepithelially in this same location to further buttress the neomeatus and hopefully prevent partial dehiscence that would result in a larger than normal meatus.
No attempt is made to secure the glans to the underlying neourethra. The remainder of glans approximation is then done using interrupted 6–0 polyglactin subepithelial sutures proximally to the corona. It is not necessary to place sutures through the epithelium of the glans, and I have seen a few patients develop suture tracks when a second layer was created.
Figure 6
Skin closures also use subepithelial 7–0 polyglactin sutures to minimize the risk of suture tracks. During circumcision the dorsal hood is incised down the midline to the level of the subcoronal collar of the inner prepuce. This point is sutured, and then the ventral shaft skin is approximated up the midline, simulating the normal median raphe. Excess skin is next excised and remaining edges sutured. When the foreskin is reconstructed the inner prepuce is first closed with interrupted sutures, then dartos is approximated, and finally the outer shaft skin is sewn, giving a three-layer closure. A Tegoderm dressing is applied and the stent is left open dripping into a diaper.
Figure 7
I recommend initially maintaining the urethral plate in all proximal hypospadias repairs, as even apparently severe ventral curvature sometimes can be straightened without transecting the plate. The skin incision should be made immediately next to the plate to minimize the risk of incorporating hair follicles into the neourethra. Similarly, the foreskin also can be preserved at the beginning of surgery as curvature is assessed, although in many patients it will be necessary to completely deglove the penis and ultimately circumcise it. My experience with foreskin reconstruction in boys with proximal defects is limited, and a desire to avoid circumcision should not outweigh the need to correct significant ventral curvature that might later impair sexual function. After degloving, the corpus spongiosum alongside the urethral plate is dissected off the underlying corpora cavernosa. This tissue later will be approximated over the neourethra as a barrier layer against fistula, and its mobilization sometimes also lessens the extent of ventral penile bending. Then an artificial erection is created; persistent mild curvature is corrected by midline dorsal plication, as described above. More severe bending next leads to dissection under the entire urethral plate, and if it still persists, to transection of the plate and, in my hands, a staged urethroplasty.
Figure 8
A midline incision of the penile aspect of the urethral plate is made to assess the ‘health’ of this tissue. In a very few cases the incised plate has appeared less supple and poorly developed, and this finding has led to excision of the unhealthy plate and a staged repair. Note that the glans is left undisturbed until this point, as even when the penile urethral plate has seemed undesirable for urethroplasty, the glandular aspect has been supple and could still be incorporated into the neourethra. When the incised plate is satisfactory, glans wings are next dissected from the urethral plate as described for distal repairs. This aspect of the plate is then incised in the midline in preparation for tubularization.
Figure 9
A 6 F stent is passed into the bladder; occasionally there may be difficulty negotiating the catheter past an enlarged utricle, and in this situation a cystoscope is introduced under vision into the bladder and a wire placed over which the stent can be manoeuvred.
To create the longer neourethra in proximal repairs, I prefer a two-layer, 7–0 polyglactin subepithelial closure, the first using interrupted sutures and the second a running suture. Care is taken to turn all visible epithelium into the neourethral lumen. Then the previously mobilized corpus spongiosum is closed, followed by coverage of the repair by a dartos pedicle flap. Glansplasty follows and then skin closure. Significant penoscrotal transposition is also corrected at this point. Next a Tegoderm dressing is applied. After proximal repairs I further immobilise the penis with a mild compression dressing consisting of a small gauze square placed onto the ventral aspect of the penis that is held in place by a second, larger Tegoderm dressing against the lower abdomen.