医脉通APP

医脉通微信
公众号
问题反馈
医脉通APP
医脉通微信
公众号
问题反馈
引 言
Barrett食管是一种食管黏膜的化生改变,以正常鳞状上皮被特化或肠化的柱状上皮所取代为特征[1–2]。肠化生具有重要的临床意义,因其可导致食管腺癌的风险增高,这种肿瘤在发达国家人群中的发病率已经大大提高。Barrett食管可伴有慢性胃食管反流病(GERD)症状群,如烧心感和反流[3]。这种伴随症状要求对所有慢性GERD患者行常规胃镜检查,以便发现Barrett食管并进一步行胃镜随访以评估其向癌症进展的程度[4]。这样的方式虽然看起来很合理,但是胃镜筛查和随访的效果如何目前仍不得而知,而且相关的医疗花费巨大且目前对其缺乏评估[5]。
临床表现
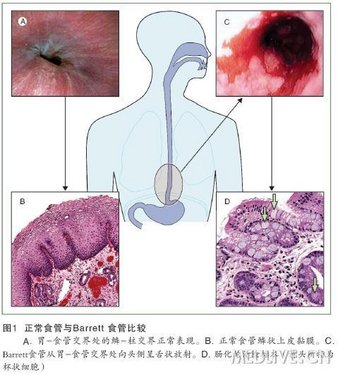
Barrett食管的诊断应满足两个标准[6–7]。首先,内镜检查应显示鳞–柱交界向头侧移位。通常情况下,鳞–柱交界应与食管最末端重叠(图1A)。食管鳞状上皮(图1B)和胃柱状上皮交界处称为Z线,原因是分界线为锯齿状。通常Z线易于分辨,因为两种上皮颜色不同:正常鳞状上皮为白色或微粉红色,而柱状上皮则是橘红色。在Barrett食管中,橘红色的上皮突起伸入食管黏膜。这种延伸可表现为舌状(图1C)和(或)累及黏膜全周(图2)。第二条诊断标准是食管活检标本中发现有肠化上皮,或包含杯状细胞的上皮(图1D)。化生上皮中杯状细胞的确认是否为诊断必需尚存在争论——美国的专业学会和权威专家要求确认杯状细胞的存在[6–8]但英国胃肠病学会不要求确认[9]。有或无杯状细胞的化生组织均被称为柱状上皮。为明确起见,内镜下具有Barrett食管表现而无组织学确认的食管上皮,应被称作内镜疑似食管化生[10]。
内镜下应测量鳞–柱交界移位的长度:长度 > 3 cm的称为长节段Barrett食管,≤3 cm的称为短节段Barrett食管[11–12]。先前研究者认为短节段Barrett食管无临床意义,但另外的一些研究已经显示,即使是短节段病变也比普通人群发生癌症的风险高[11,13]。因此,目前关于Barrett食管最普遍的定义是食管任何长度的包含杯状细胞的橘红色黏膜。
在正常外观的Z线活检标本中出现杯状细胞或肠化是否可导致食管腺癌或胃贲门腺癌的风险升高?在有GERD症状群但内镜下无Barrett食管证据的患者中,大约20%患者的Z线活检标本中存在肠化[14]。大量的此类患者被认为有连续而平直的鳞–柱交界线。无内镜下异常或反流症状史而接受常规胃镜检查的患者中,10%~17%的患者在其活检标本中发现有肠化上皮[15]。该病变的病因和自然史尚不明确,但看起来似乎为良性,其在贲门进展为不典型增生的概率比较低[16]。在正常Z线出现杯状细胞或肠化上皮的患者是否应该常规进入内镜随访计划也不明确。考虑到这种病变表现多为良性,且食管腺癌和贲门癌较少见,一般认为这类患者癌变的风险较低。因此,不推荐对具有GERD症状群但胃–食管交界外观正常的患者行常规内镜活检。
流行病学
Barrett食管在普通人群尤其在有慢性反流症状的人群中患病率很高,但也有一些患者是无症状性反流。内镜筛查策略的制定和对癌变风险的理解部分依赖于普通人群中Barrett食管的患病率。1990年,美国明尼苏达州Olmsted县通过大约1000例随机尸检得到的Barrett食管患病率为376/10万人[23]。这一数字是该县临床诊断病例数的21倍,这表明有许多Barrett食管患者根本未被发现。瑞典一项严密的调查研究[24]发现,成人Barrett食管的总体患病率为1.6%,其中大约1/3为长节段性。超过40%的Barrett食管患者报告无反流疾病。对于无症状患者,研究者未能在人口统计学或症状问卷调查数据中一致地确定其Barrett食管患病的危险因素。在同时行结肠癌内镜筛查的体检人群中,Barrett食管的患病率在美国中西部人群[25]的5.6%到老年人[26]和退伍军人[27]的15%~25%之间波动。
尽管Barrett食管在普通人群中的患病率很高,但在因慢性反流症状而接受胃镜检查的患者中更高,可达5%~15%[28–31]。Barrett食管的患病风险及其节段的长度随食管远端酸暴露量的增多而增加,两者也都与食管裂孔疝的存在及其大小相关[32–35]。遗憾的是,GERD症状群不是Barrett食管的预测因子[28,36],经有研究发现烧心样症状的严重程度与Barrett食管关系不大或无关[37]。然而,反流症状的频率和长期性(总的反流年数)是Barrett食管中比症状严重程度更好的预测因子[3,38]。
对慢性烧心样症状患者而言,Barrett食管人口统计学方面的预测因子包括性别、年龄和种族。即使反流症状的严重程度得到控制,白种人的患病风险也较高,老年人也是如此[24,31,36]。对该病易感的原因尚不清楚,而且目前Barrett食管是否有遗传易感性也尚不明确[39]。其他潜在的危险因素包括吸烟和饮食习惯[32,40]。与食管鳞状细胞癌不同的是,酗酒和慢性吸烟是最弱的危险因素[24,40–42]。应用非固醇类抗炎药(NSAID)是否可以降低Barrett食管的风险目前尚不明确,尽管一些队列研究和病例对照研究数据显示既往的慢性NSAID暴露可降低Barrett食管患病率,但这些数据易受混杂的一些未被测量的卫生习惯所影响,最近一项试图证明环氧合酶2(COX-2)抑制剂对Barrett食管患者抗癌效果的研究未获成功[43]。
发病机制
Barrett食管是否具有遗传性目前尚不清楚。几项研究报道显示,Barrett食管患者的一级亲属中患该病的比例高于随机检查所预计的比例[39,44],但未鉴定出相关基因,尽管这些数据可能存在检测偏倚。Barrett食管和食管腺癌患病的风险均与体重指数(BMI)有关,这经被大家所熟知。BMI升高与GERD症状群和糜烂性食管炎的风险升高有统计学关联[45],这进而提高了GERD并发症发生的风险[15],甚至轻度BMI升高都可增加反流症状群的发生[46]。一项横断面研究估计Barrett食管患者腹部内脏组织平均为对照组的1.5倍[47]。一些病例对照研究结果也显示了向心性肥胖在Barrett食管发生中的重要性[48–49]。一项基于人群的病例对照研究发现腰-臀比升高与Barrett食管强相关[49]。事实上,当研究者控制这个比例后,BMI和Barrett食管的关系几乎完全消失,这表明BMI引起的Barrett食管的高风险是通过向心性肥胖介导的。
向心性肥胖增加Barrett食管发生的可能途径是什么?一个解释是向心性肥胖者易患食管裂孔疝[50–51]。而且肥胖增加了胃内压力,促进了反流发生。更引人注目的解释或许是激素学说。向心性肥胖患者有高浓度的胰岛素和胰岛素样生长因子,而后者可促进细胞增殖并决定细胞分化。患者具有多种脂肪细胞因子,这些肽可介导细胞炎症和凋亡。
鉴于在慢性反流患者中Barrett食管患病率升高,一些学者猜想起始事件可能是偶发的腐蚀性反流,这种反流可侵蚀正常食管上皮并使其增殖为柱状上皮。对狗[52]重复注射组胺引起的高酸量可导致上皮化生和Barrett食管形成。临床研究已经确认Barrett食管患者存在严重的GERD[53]。一般情况,这些患者比糜烂性食管炎或非糜烂性胃食管反流病的食管下段括约肌压力下降更明显,食管运动障碍更明显,超过90%的患者有pH明显异常[53]。其他研究者报道了Barrett食管患者有长期腐蚀性浓度的胃酸暴露(pH < 3.0或2.0)[54],长节段Barrett食管有较高程度的近端酸反流[34],Barrett食管患者的裂孔疝发生率较高(Barrett食管患者:76% vs反流患者:36%)[32]。胃内出现胆汁和胆汁反流(通常伴随酸反流)在Barrett食管患者比在非Barrett食管的GERD患者中更常见[55]。
这些研究结果表明酸和胆汁在Barrett食管发生中可能存在协同作用,虽然胆汁可能单独不起作用[56]。对食管细胞的实验室研究支持这个假说,研究表明短期胆汁酸暴露和低pH值可导致氧化应激和DNA损伤[57]。这些变化可能是Barrett食管和肿瘤发生的基础。动物模型表明,解剖学改变导致了致病量的酸和胆汁反流,最终导致了食管特化上皮发生[58–59]。这种动物模型中许多动物因持续的上皮损伤而导致了癌变。
另一个重要的环境因素可能是Hp感染。这种感染可能使胃内酸度降低,通过产生大量的氨和(或)破坏胃壁细胞造成严重的胃体炎而减少酸排出[60]。感染Hp的CagA+菌株与高级别胃炎及发展为胃萎缩和肠化生的倾向有关[61]。在美国和欧洲尤其是在东亚,Hp感染的存在可防止发生糜烂性食管炎甚至Barrett食管[62]。在发达国家Hp感染率逐渐下降的同时GERD并发症(包括Barrett食管)的发病率却在上升。
然而,宿主因素(相关研究较少)也可能具有重要意义,因为许多患者会发生严重的复发性糜烂性食管炎,但却不发生Barrett食管。上皮化生造成细胞间紧密连接蛋白成分的显著性变化,导致了Barrett食管患者比健康人群的食管黏膜更耐酸[64]。因此,Barrett食管的发生实际上可能代表着短期适应,从而减少了慢性反流的并发症,如出血和狭窄。
Barrett食管形态学变化的分子学基础正在被阐明。在炎症反应(包括细胞因子基因多态性)、DNA修复和化学解毒中起重要作用的基因多态性与Barrett食管的发生或发展有关[65–67]。由于可遗传性弱,且与任何普遍认可的模式不一致,因此认为Barrett食管可能是一个多基因疾病,而不是单个基因的突变。对比研究Barrett食管和鳞状组织中的基因表达,提示在化生过程中存在不同的细胞激活途径[68–70]。例如,CDX2基因似乎在胃肠细胞的分化过程中非常重要[68],过表达该基因的转基因动物可发生异常肠上皮化生,而敲除该基因的动物在小肠可出现异常的鳞状组织岛。一些数据表明,表观遗传变化在可能促进Barrett食管发生的异常基因表达中起部分作用。例如,CDX2启动子区域的去甲基化可能允许这一基因在先前静态的细胞系中被表达,从而诱导子代细胞肠化[69]。这种机制可能是遗传机制和环境暴露之间的一种联系。例如,在动物模型中,上皮细胞暴露于十二指肠内容物可影响CDX2的表达[70]。
Barrett食管来源的祖细胞目前还不清楚。候选者包括存在于上皮黏膜下层腺体或基底层之间上皮细胞的祖细胞、骨髓来源的干细胞或转分化的鳞状细胞[71]。有鳞状上皮和柱状上皮细胞标记的多层上皮可能先于Barrett食管发生[72]。动物模型表明,Barrett食管可以在不直接与柱状上皮接连的情况下发生[58],从而使柱状细胞的迁移似乎不可能形成。
诊 断
1 标准内镜检查
内镜检查是Barrett食管常规的诊断方法,但结果需经内镜活检标本的组织病理学检查确认。其他方法如钡餐透视或CT检查都没有足够的敏感性。有慢性反流症状的患者应该在接受PPI抑酸治疗至少4周后接受Barrett食管的上消化道内镜筛查。因为虽然PPI预处理将减少胃镜检查中糜烂性食管炎的检出率,但食管末端的炎症可能会掩盖Barrett食管。严重的糜烂性食管炎可使多达12%的短节段Barrett食管漏检[73]。在内镜检查中,移位的鳞–柱交界长度应该被测量。鳞–柱交界近端延伸部分往往为环状,但也可能是舌状的柱状黏膜,尤其是在短节段Barrett食管中。为确定Barrett食管的最长界限,应该在内镜下确定胃皱襞的最近端。此外,黏膜毛细血管循环的特征模式可以在窄带内镜下进行确认[74]。
一个国际工作组提出并验证了一种Barrett食管的内镜分类系统[75]。布拉格C和M标准是在最小充气情况下,评估胃食管交界处以上内镜所见的Barrett食管的环周部分长度(C)和最远(M)范围(图 2)。观察者间评估C和M的范围的总体可靠性系数分别为0.95和0.94。内镜辨认≥1 cm的Barrett食管总体可靠性系数为中度(0.72),但对1 cm以下的Barrett食管则较差(0.22)。
Barrett食管的确诊应在可疑Barrett食管的全段进行随机活检,对活检标本进行HE染色后检查,并确定含杯状细胞的肠上皮化生。对于不确定的病例,可用pH值为2.5的Alcin蓝染色使杯状细胞显示[76]。一些研究者[77]建议,应取8处随机活检标本以提高肠上皮化生的检出率。内镜发现不同长度的呈柱状表现的黏膜,其组织学确认率不同,内镜可疑的短节段Barrett食管仅有大约25%被确认,长节段Barrett食管约有44%~80%被确认[78]。最初的胃镜检查未确认肠化的患者中有超过20%的患者在后来的胃镜随访中发现了肠化[79],可能是因为取材误差或在最初的胃镜检查后才发生肠化。
遗憾的是,Barrett食管组织学分级的可靠性较差。病理学专家诊断不典型增生程度的一致性经常为低至中度(κ = 0.2~0.6),并且在训练后仅略有改善[80–81]。造成这种困难的主要原因在于提供的活检标本太小和缺乏不典型增生程度分级的共识,此外在同时存在食管炎的患者中,判断不典型增生的分级是困难的,这些患者多为慢性反流症状患者。
关于内镜筛查方案(目的是从慢性GERD患者中识别出Barrett食管患者)与内镜随访方案(目的是监测Barrett食管患者是否向癌症进展)应用的讨论仍在继续。几个专业组织已经发布了内镜筛查和内镜随访指南,这些指南提供了推荐的定期内镜检查的时间间隔(附表)。这些指南的倡导者注意到食管腺癌的发病率的快速增长,以及联系慢性GERD症状与Barrett食管发生及癌变风险增加的有力证据。然而,质疑者指出,存在慢性反流症状而需要进行筛查的患者数量很大,而GERD患者个体癌变的绝对风险很小;筛查花费巨大,而且该方法的效果未经证实[2]。
尽管尚无直接证据支持内镜筛查和内镜随访,但这种做法在美国和英国经相当普遍[82]。内镜筛查和内镜随访的成本–效果比尚不清楚,而且依赖于不明确的因素,如诊断Barrett食管方法的准确性、Barrett食管癌变的风险以及内镜和组织病理学检查的费用[83–84]。有分析认为,尽管一次内镜筛查的成本–效果比较好,在活检结果为Barrett食管而无不典型增生的患者内镜随访中的成本–效果比差,而且额外花费几千美元仅增加很短的预期寿命[85]。
为取代对慢性GERD患者的传统内镜检查经做了很多努力。不依赖内镜的球囊细胞学检查诊断杯状细胞的成功率令人失望,在63例患者中只有24%被检出[86]。摩擦性更高的球囊可能会产生较高的成功率。另一种替代方法是小口径经鼻内镜。此方法是在不用麻醉剂的情况下,用5~6 mm的胃镜通过鼻孔到咽部,并下到食管进行检查。在一项随机交叉研究中[87],对121例患者进行Barrett食管内镜筛查和随访,发现传统的内镜(26%)和非麻醉的小口径内镜(30%)检出的Barrett食管的患病率相似;两种方法的一致性为中度(κ = 0.591)。每种方法发现4例低级别不典型增生,在同一病例中两者一致,尽管小口径内镜夹取的组织样本较小。超过70%的患者倾向于小口径内镜,因为此方法可以不需要监护和恢复时间,也不耽误工作时间,不需要司机代驾。这种方法的缺点是缺少病理学确诊所需要的足够的组织标本。
另一种被评估的方法是胶囊内镜。它是一种特殊设计的胶囊,当通过食管时,胶囊两端的照相设备可获得大量照片(最多为14帧/s)。在一项单中心前瞻性研究[88]中,90例患者接受了Barrett食管的检查或监测,胶囊内镜的敏感性为67%,特异性为84%,诊断出了被活检确诊的14/21例。对短节段和长节段Barrett食管的敏感性相似。然而,这一非侵入性技术的诊断准确性有限,照片上过多的碎片或气泡使Z线变得模糊,只有少量照片中胃–食管交界清晰可见。法国研究者在对89例患者的一项研究中,观察到了胶囊内镜有所改善的操作特性[89],他们报告胶囊内镜有良好的特异性和较佳的阴性预测值,但敏感性不理想。在目前情况下,这项技术在慢性GERD患者中检测Barrett食管的成本–效果比不如标准内镜[90–91]。
提高常规内镜检查和监测效果及成本–效果比的方法是提高检查的准确性。随机活检标本只能包括病变的一小部分。目前正在开发的一些技术,可对大面积黏膜进行光学扫描以寻找可能的病变,并准确有效地识别可疑区域以进一步定性。
2 先进的内镜成像
色素内镜是一项简单的技术,是应用化学物质通过选择性摄取(用亚甲蓝或Lugol液进行活性染色)或增强黏膜表面的模式(用靛蓝胭脂红和乙酸进行对比染色)而改善黏膜表面特征。在这些染色方法中,亚甲蓝最为常用,可使非不典型增生肠上皮化生染为蓝色,但对有高级别不典型增生或癌变的黏膜不染色[92]。结果有好有坏,前瞻性交叉研究表明,亚甲蓝色素内镜效果并不佳,在某些情况下比随机四象限活检检测不典型增生更差[93–94]。与此技术相关的问题包括难于获取全面的黏膜层、需要额外喷洒染料的时间,以及无法检测黏膜表面的血管模式。对比剂如结晶紫、靛蓝胭脂红和醋酸,结合高分辨率内镜可提高黏膜模式的检测效果[95],但目前尚未被广泛使用。
另一种扫描大面积的黏膜以寻找可能的癌变的方法是窄带成像。该项技术通过缩小白光带宽,将其过滤为两种主要颜色(蓝色和绿色),以便被黏膜及黏膜下血管更好地吸收而提高对比度(图3)。窄带成像结合高分辨率内镜可提供Barrett食管节段黏膜和血管表面形态的详细图像,并识别非不典型增生肠上皮化生、高级别不典型增生和早期癌的特征性模式[96]。在一项对51例Barrett食管患者的研究中[97],其中7例为高级别不典型增生,窄带成像检测非不典型增生肠上皮化生的敏感性为93.5%,检测高级别不典型增生不规则或扭曲模式的敏感性为100%,特异性为98.7%。窄带成像无法区分肠上皮化生和低级别不典型增生。然而,一项荷兰研究[98]未能表明,增加窄带成像或活性染色可提高标准内镜对不典型增生的识别。
另一种改善标准内镜方法的是自体荧光技术,它使用蓝光检测组织自然发生的荧光。肿瘤黏膜在Barrett食管中往往出现蓝紫色,而非不典型增生组织显示为绿色[99]。因此,窄带成像或自体荧光成像结合标准内镜,可使与高级别不典型增生或癌有关的隐性或轻微的黏膜异常得到准确的观察,而不会出现色素内镜的不方便或混乱的结果。
光学相干断层扫描可提供活体组织的高分辨率横断面图像。该技术和超声显像类似,但它使用的是红外线而不是声能,其分辨率为高频超声的10倍以上,尽管其最大检测深度低于超声显像[100]。在一项对33例患者的前瞻性双盲研究中[101],这项技术对于在Barrett食管患者中检测异常增生的准确率为78%。然而,在4名资深内镜专家中诊断准确率从56%至98%不等[101]。激光共聚焦显微镜可以使黏膜放大1000倍以上,可描述细胞的结构。在一项对63例Barrett食管及并发相关癌变的患者研究[102]中显示,激光共聚焦显微镜检测癌变的准确性为97.4%。潜在的意义是,这些新技术可以提供真正的光学活检标本,并减少或免除对黏膜活检标本的处理和解释的需要。
治 疗
与普通人群相比,Barrett食管患者的生活质量显著下降[103]。患者往往会误解并高估该病的癌症发生率[104]。一项美国研究[105]显示,在确诊为Barrett食管的患者中,尽管预期寿命和同年龄、同性别对照组相似,但其人身保险费增加了100%以上。考虑内镜下Barrett食管筛查的患者应在筛查前被告知这些风险。
队列研究显示,大多数Barrett食管患者没有从非不典型增生疾病或短暂的低级别不典型增生继续进展[20]。在大多数长期研究中,进展为高级别不典型增生或癌的患者远少于10%[20]。为此,推荐组织中达成的共识是,非不典型增生或低级别不典型增生的Barrett患者应保守治疗,定期行内镜监测[7,9]。
围绕高级别不典型增生患者最适当的治疗方案引起了激烈争论,因为其进展为癌症的风险大大增加,在一些研究中其每年的癌变率为4%、2.2%和11.8%[20,106–107]。因此,对这类患者往往需要考虑干预。通常采用3种策略,即外科食管切除术、频繁的内镜随访观察和内镜治疗。
外科手术的倡导者注意到在食管切除标本中检出了一些先前未被发现的微小癌灶,发生这种情况的风险比较高,外科系列研究报道在这些标本中隐匿性癌的发现率为10%~50%[108–109]。然而,在这些研究中,术前活检情况未得到较好描述,其他权威学者也质疑这些侵袭性癌的定义[110]。另外,食管切除术对术者水平高度依赖。与手术病死率≤5% [111–112]的专科医疗中心相比,手术例数少的中心食管切除术的并发症率和病死率较高,据报道其在术后30 d的病死率高达20%[113]。因此,一些中心已经改变了策略,采取频繁内镜随访(第1年每3个月一次,第2年每年两次,此后每年一次),只对直接向癌症进展的患者进行干预。在对75例患者运用该策略平均处理7.8年后,84%未发生癌变[20]。而其余的16%癌变患者几乎全部因为早期发现而得到成功干预。只有1例失访数年的患者发生了转移癌。
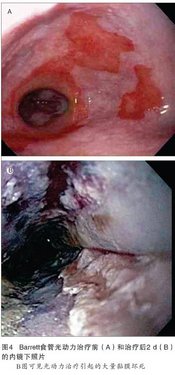
Barrett食管治疗方面发展最迅速的也许是内镜治疗,即通过内镜切除(内镜下黏膜切除术或内镜下黏膜剥离术)或食管内壁消融。所有这些方法的依据是,最初观察到在破坏食管内壁后采用高剂量抑酸治疗,通常会导致鳞状上皮再生[114–115]。虽然新生的鳞状上皮细胞是否有恶性潜能尚未完全了解,但这种逆转大大降低了食管腺癌的风险[21]。内镜消融上皮的治疗方法有多极电凝[116]、激光治疗[117]、氩离子凝固[118–119]、光动力疗法[120–121]、喷洒液氮的冷冻疗法[122]及射频消融[123]。通过比较这些疗法,推荐某一疗法的证据尚不充分,而且各种疗法治疗后发生癌症的相对可能性也未得到评估。光动力疗法(图4),是给予光敏物质后对食管进行激光治疗。一项多中心随机盲法对照试验[21]证明,可使高级别不典型增生患者癌症的发生率减少50%以上(从28%下降至13%)。有研究显示,射频消融术可有效消除非不典型增生[124]和高级别不典型增生[125]Barrett食管。内镜切除部分或全部的Barrett食管组织可用于消融治疗前消除结节,或作为一种独立的治疗方法[126–127]。
高级别不典型增生Barrett食管的最佳处理方法依赖于患者自身特点、患者喜好及当地的专业技术水平。在并存多种疾病的患者中,内镜消融或内镜随访可使其达到最佳的预期寿命。对存在广泛性、多灶性高级别不典型增生的年轻患者,外科手术或内镜治疗比频繁的内镜监测更适宜。鉴于对各种处理策略进行比较的数据较少,处理高级别不典型增生的教条式方法并不可取。
化学药物的使用对预防Barrett食管发生或进展至不典型增生是否有作用?流行病学研究表明,长期使用NSAID的患者食管癌发生率为普通人群的一半[128],因此NSAID的使用已经被假定可减少Barrett食管的发病率或至少推迟其进展为癌症。然而遗憾的是,最近报道的随机对照试验表明,200 mg/d的塞来昔布(一种COX-2的选择性NSAID)对伴低级别或高级别不典型增生的Barrett食管未表现出防止疾病进展的保护效应[43]。大量的观察数据显示,长期PPI抑酸治疗可延缓Barrett食管向不典型增生进展[129–130]。然而,目前还没有令人信服的前瞻性研究数据,而且抑酸药物的最佳剂量目前尚不清楚。此外,由于Barrett食管经常是在对慢性GERD症状患者行内镜检查时发现的,而这些症状往往需要PPI才能得到有效控制,因此在不考虑化学预防的情况下也会给予这种维持治疗。截至目前,超过控制症状所需要的大剂量PPI治疗,并未被证明可降低癌症风险,因此仅为了化学预防而应用超治疗剂量是不合理的。
抗反流手术适用于不耐受药物或对药物治疗完全无反应的GERD患者。这些外科手术是否比长期抑酸药物治疗更能减少Barrett食管患者癌变的风险?虽然关于这个问题的研究数据存在分歧,但总体而言,抗反流手术不应作为一种抗癌变措施。101例Barrett食管患者被随机分组接受抗反流手术或抑酸药物治疗,平均随访5年,两组间疾病进展率没有差异[131]。同样,荟萃分析结果显示,Barrett食管患者的癌症发生率在手术组和药物治疗组之间没有差异[132]。然而,在这些分析中可能未考虑到手术类型和成功率、医疗处理的严格性和病例选择因素等重要细节。
未来研究方向
Barrett食管的最佳处理策略需要进一步研究。也许最重要的是需要进行风险分层。目前,我们不能充分预测有慢性烧心样症状的众多患者中哪些患者将会发生Barrett食管,也许更为重要的是,哪些患者将从Barrett食管进展到不典型增生和癌症。采用内镜活检进行组织学分析,以评估不典型增生的程度和癌变风险远不够完善,而且重复性差。利用上消化道内镜进行筛查和监测随访,不仅费用昂贵,而且必须在专业的医疗中心进行。面临Barrett食管风险(即患有慢性烧心样症状)的人群数量巨大,但食管腺癌发病率虽在增加但仍比较低[133]。更复杂的是,发展为食管癌的患者中多达40%的患者仅有轻微反流症状[134]。
尽管这种情况似乎令人沮丧,但事态发展表明医疗会获得改善。对食管腺癌发病机制的众多研究经发现了一些疾病进展的潜在生物标志物,如TP53基因突变、非整倍体、细胞周期蛋白A免疫阳性和α甲基辅酶A消旋酶的表达[135–137]。巢式病例对照研究的初步结果表明,这些生物标志物预测癌症风险的敏感性和特异性可能比传统的组织学更高[138]。目前还没有发现可以描述疾病进展的可靠生物标志物,而且这些生物标志物的操作特征尚未充分阐明。然而,可能最终会发现一组生物标志物可以对高危患者提供足够的预后信息,也许同样重要的是,有了这些生物标志物就可以免除那些极低危患者接受进一步的内镜检查和其他处理的需要。筛查和随访也将得到发展,改进的设备可以使内镜评估更为容易,并且使其成本更低廉。
归根底,发展一个微创的生物标志物(如血清或痰测试),可能会使内镜筛查被淘汰。因为有些患者会反复发生严重糜烂性食管炎而没有发展为Barrett食管,对使食管黏膜损害患者易发生柱状上皮组织化生的基因的识别极为有用。候选基因的等位基因发生率的研究正在进行。这些遗传信息也有助于确定慢性烧灼样症状的患者中哪些患者具有患Barrett食管和癌变的风险。
改进的内镜治疗将可能继续减少不典型增生患者对食管切除术的需要。消融技术的损伤性在降低,耐受性在提高,可能将获得足够的数据表明其应用在非不典型增生疾病中既可降低癌变的风险又可降低成本(因为它减少了内镜随访的需要)。对Barrett食管潜在的初级和次级化学预防的深入了解,可能使NSAID、抑酸药物和其他药物被适当地应用。欧洲一项大型研究[139]探索了小剂量阿司匹林和PPI联合及单独应用在Barrett食管预防中的作用,可能会阐明这些药物在Barrett食管预防中的作用及最佳剂量。
(王晓君 译)
参 考 文 献
[1]Spechler SJ. Barrett’s esophagus. N Engl J Med, 2002, 346: 836–42
[2]Shaheen N, Ransohoff DF. Gastroesophageal reflux, Barrett esophagus, and esophageal cancer: scientific review. JAMA, 2002, 287: 1972–81
[3]Eisen GM, Sandler RS, Murray S, et al. The relationship between gastroesophageal reflux disease and its complications with Barrett’s esophagus. Am J Gastroenterol, 1997, 92: 27–31
[4]Sampliner RE and the Practice Parameters Committee of the American College of Gastroenterology. Updated guidelines for the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol, 2002, 97: 1888–95
[5]Shaheen NJ, Provenzale D, Sandler RS. Upper endoscopy as a screening and surveillance tool in esophageal adenocarcinoma: a review of the evidence. Am J Gastroenterol, 2002, 97: 1319–27
[6]Sharma P, McQuaid K, Dent J, et al. A critical review of the diagnosis and management of Barrett’s esophagus: the AGA Chicago Workshop. Gastroenterology, 2004, 127: 310–30
[7]Wang KK, Sampliner RE, the Practice Parameters Committee of the American College of Gastroenterology. Updated guidelines 2008 for the diagnosis, surveillance and therapy of Barrett’s esophagus. Am J Gastroenterol, 2008, 103: 788–97
[8]Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. ASGE guideline: the role of endoscopy in the surveillance of premalignant conditions of the upper GI tract. Gastrointest Endosc, 2006, 63: 570–80
[9]Playford RJ. New British Society of Gastroenterology (BSG) guidelines for the diagnosis and management of Barrett’s oesophagus. Gut, 2006; 55: 442
[10]Vakil N, van Zanten SV, Kahrilas P, et al. and the Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol, 2006, 101: 1900–20
[11]Sharma P, Morales TG, Bhattacharyya A, et al. Dysplasia in short-segment Barrett’s esophagus: a prospective 3-year follow-up. Am J Gastroenterol, 1997, 92: 2012–16
[12]Spechler SJ. Short and ultrashort Barrett’s esophagus—what does it mean? Semin Gastrointest Dis, 1997, 8: 59–67
[13]May A, Gossner L, Pech O, et al. Intraepithelial high-grade neoplasia and early adenocarcinoma in short-segment Barrett’s esophagus (SSBE): curative treatment using local endoscopic treatment techniques. Endoscopy, 2002, 34: 604–10
[14]Spechler SJ, Zeroogian JM, Antonioli DA, et al. Prevalence of metaplasia at the gastro-oesophageal junction. Lancet, 1994, 344: 1533–36
[15]Wallner B, Sylvan A, Stenling R, et al. The Z-line appearance and prevalence of intestinal metaplasia among patients without symptoms or endoscopical signs indicating gastroesophageal reflux. Surg Endosc, 2001, 15: 886–89
[16]Morales TG, Camargo E, Bhattacharyya A, et al. Long-term follow-up of intestinal metaplasia of the gastric cardia. Am J Gastroenterol, 2000, 95: 1677–80
[17]O’Connor JB, Falk GW, Richter JE. The incidence of adenocarcinoma and dysplasia in Barrett’s esophagus: report on the Cleveland Clinic Barrett’s Esophagus Registry. Am J Gastroenterol, 1999, 94: 2037–42
[18]Drewitz DJ, Sampliner RE, Garewal HS. The incidence of adenocarcinoma in Barrett’s esophagus: a prospective study of 170 patients followed 4·8 years. Am J Gastroenterol, 1997, 92: 212–15
[19]Shaheen NJ, Crosby MA, Bozymski EM, et al. Is there publication bias in the reporting of cancer risk in Barrett’s esophagus? Gastroenterology, 2000, 119: 333–38
[20]Schnell TG, Sontag SJ, Chejfec G, et al. Long-term nonsurgical management of Barrett’s esophagus with high-grade dysplasia. Gastroenterology, 2001, 120: 1607–19
[21]Overholt BF, Lightdale CJ, Wang KK, et al, on behalf of the International Photodynamic Group for High-Grade Dysplasia in Barrett’s Esophagus. Photodynamic therapy with porfimer sodium for ablation of high-grade dysplasia in Barrett’s esophagus: international, partially blinded, randomized phase III trial. Gastrointest Endosc, 2005, 62: 488–98
[22]Weston AP, Sharma P, Topalovski M, et al. Long-term follow-up of Barrett’s high-grade dysplasia. Am J Gastroenterol, 2000, 95: 1888–93
[23]Cameron AJ, Zinsmeister AR, Ballard DJ, et al. Prevalence of columnar-lined (Barrett’s) esophagus. Comparison of population-based clinical and autopsy findings. Gastroenterology, 1990, 99: 918–22
[24]Ronkainen J, Aro P, Storskrubb T, et al. Prevalence of Barrett’s esophagus in the general population: an endoscopic study. Gastroenterology, 2005, 129: 1825–31
[25]Rex DK, Cummings OW, Shaw M, et al. Screening for Barrett’s esophagus in colonoscopy patients with and without heartburn. Gastroenterology, 2003, 125: 1670–77
[26]Ward EM, Wolfsen HC, Achem SR, et al. Barrett‘s esophagus is common in older men and women undergoing screening colonoscopy regardless of reflux symptoms. Am J Gastroenterol, 2006, 101: 12–17
[27]Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology, 2002, 123: 461–67
[28]Voutilainen M, Sipponen P, Mecklin JP, et al. Gastroesophageal reflux disease: prevalence, clinical, endoscopic and histopathological findings in 1128 consecutive patients referred for endoscopy due to dyspeptic and reflux symptoms. Digestion, 2000, 61: 6–13
[29]Conio M, Filiberti R, Blanchi S, et al. Risk factors for Barrett’s esophagus: a case-control study. Int J Cancer, 2002, 97: 225–29
[30]Lin M, Gerson LB, Lascar R, et al. Features of gastroesophageal reflux disease in women. Am J Gastroenterol, 2004, 99: 1442–47
[31]Westhoff B, Brotze S, Weston A, et al. The frequency of Barrett’s esophagus in high-risk patients with chronic GERD. Gastrointest Endosc, 2005, 61: 226–31
[32]Avidan B, Sonnenberg A, Schnell TG, et al. Hiatal hernia and acid reflux frequency predict presence and length of Barrett’s esophagus. Dig Dis Sci, 2002, 47: 256–64
[33]Cameron AJ. Barrett’s esophagus: prevalence and size of hiatal hernia. Am J Gastroenterol, 1999, 94: 2054–59
[34]Fass R, Hell RW, Garewal HS, et al. Correlation of oesophageal acid exposure with Barrett’s oesophagus length. Gut, 2001, 48: 310–13
[35]Oberg S, DeMeester TR, Peters JH, et al. The extent of Barrett’s esophagus depends on the status of the lower esophageal sphincter and the degree of esophageal acid exposure. J Thorac Cardiovasc Surg, 1999, 117: 572–80
[36]Eloubeidi MA, Provenzale D. Clinical and demographic predictors of Barrett’s esophagus among patients with gastroesophageal reflux disease: a multivariable analysis in veterans. J Clin Gastroenterol, 2001, 33: 306–09
[37]Locke GR, Zinsmeister AR, Talley NJ. Can symptoms predict endoscopic findings in GERD? Gastrointest Endosc, 2003, 58: 661–70
[38]Conio M, Filiberti R, Blanchi S, et al. Risk factors for Barrett’s esophagus: a case-control study. Int J Cancer, 2002, 97: 225–29
[39]Chak A, Lee T, Kinnard MF, et al. Familial aggregation of Barrett’s oesophagus, oesophageal adenocarcinoma, and oesophagogastric junctional adenocarcinoma in Caucasian adults. Gut, 2002, 51: 323–28
[40]Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology, 2002, 123: 461–67
[41]Gray MR, Donnelly RJ, Kingsnorth AN. The role of smoking and alcohol in metaplasia and cancer risk in Barrett’s columnar lined oesophagus. Gut, 1993, 34: 727–31
[42]Ritenbaugh C, Sampliner R, Aickin M, et al. Risk factors for Barrett’s oesophagus: a life history approach to behavioural assessment in the distant past. Eur J Cancer Prev, 1995, 4: 459–68
[43]Heath EI, Canto MI, Piantadosi S, et al. Secondary chemoprevention of Barrett’s esophagus with celecoxib: results of a randomized trial. J Natl Cancer Inst, 2007, 99: 545–57
[44]Romero Y, Cameron AJ, Schaid DJ, et al. Barrett’s esophagus: prevalence in symptomatic relatives. Am J Gastroenterol, 2002, 97: 1127–32
[45]Hampel H, Abraham NS, El-Serag HB. Meta-analysis: obesity and the risk for gastroesophageal reflux disease and its complications. Ann Intern Med, 2005, 143: 199–211
[46]acobson BC, Somers SC, Fuchs CS, et al. Body-mass index and symptoms of gastroesophageal reflux in women. N Engl J Med, 2006, 354: 2340–48
[47]El-Serag HB, Kvapil P, Hacken-Bitar J, et al. Abdominal obesity and the risk of Barrett‘s esophagus. Am J Gastroenterol, 2005, 100: 2151–56
[48]Corley DA, Kubo A, Levin TR, et al. Abdominal obesity and body mass index as risk factors for Barrett’s esophagus. Gastroenterology, 2007, 133: 34–41
[49]Edelstein ZR, Farrow DC, Bronner MP, et al. Central adiposity and risk of Barrett’s esophagus. Gastroenterology, 2007, 133: 403–11
[50]Wilson LJ, Ma W, Hirschowitz BI. Association of obesity with hiatal hernia and esophagitis. Am J Gastroenterol, 1999, 94: 2840–44
[51]Stene-Larsen G, Weberg R, Frøyshov Larsen I, et al. Relationship of overweight to hiatus hernia and reflux oesophagitis. Scand J Gastroenterol, 1988, 23: 427–32
[52]Bremner CG, Lynch VP, Ellis FH Jr. Barrett’s esophagus: congenital or acquired? An experimental study of esophageal mucosal regeneration in the dog. Surgery, 1970, 68: 209–16
[53]Iascone C, DeMeester TR, Little AG, et al. Barrett’s esophagus: functional assessment, proposed pathogenesis, and surgical therapy. Arch Surg, 1983, 118: 543–49
[54]Stein HJ, Hoeft S, DeMeester TR. Functional foregut abnormalities in Barrett’s esophagus. J Thorac Cardiovasc Surg, 1993, 105: 107–11
[55]Vaezi MF, Richter JE. Role of acid and duodenogastroesophageal reflux in gastroesophageal reflux disease. Gastroenterology, 1996, 111: 1192–99
[56]Avidan B, Sonnenberg A, Schnell TG, et al. Gastric surgery is not a risk for Barrett’s esophagus or esophageal adenocarcinoma. Gastroenterology, 2001, 121: 1281–85
[57]Dvorak K, Payne CM, Chavarria M, et al. Bile acids in combination with low pH induce oxidative stress and oxidative DNA damage: relevance to the pathogenesis of Barrett’s oesophagus. Gut, 2007, 56: 763–71
[58]Buttar NS, Wang KK, Leontovich O, et al. Chemoprevention of esophageal adenocarcinoma by COX-2 inhibitors in an animal model of Barrett’s esophagus. Gastroenterology, 2002, 122: 1101–12
[59]Chen X, Li N, Wang S, et al. Aberrant arachidonic acid metabolism in esophageal adenocarcinogenesis, and the effects of sulindac, nordihydroguaiaretic acid, and alpha-difluoromethylornithine on tumorigenesis in a rat surgical model. Carcinogenesis, 2002, 23: 2095–102
[60]Labenz J, Malfertheiner P. Helicobacter pylori in gastro-oesophageal reflux disease: causal agent, independent or protective factor? Gut, 1997; 41: 277–80
[61]Maaroos HI, Vorobjova T, Sipponen P, et al. An 18-year follow-up study of chronic gastritis and Helicobacter pylori association of CagA positivity with development of atrophy and activity of gastritis. Scand J Gastroenterol, 1999, 34: 864–69
[62]Vaezi MF, Falk GW, Peek RM, et al. CagA-positive strains of Helicobacter pylori may protect against Barrett’s esophagus. Am J Gastroenterol, 2000, 95: 2206–11
[63]El-Serag HB, Sonnenberg A. Opposing time trends of peptic ulcer and reflux disease. Gut, 1998, 43: 327–33
[64]Jovov B, Van Itallie CM, Shaheen NJ, et al. Claudin-18: a dominant tight junction protein in Barrett’s esophagus and likely contributor to its acid resistance. Am J Physiol Gastrointest Liver Physiol, 2007, 293: G1106–13
[65]Siahpush SH, Vaughan TL, Lampe JN, et al. Longitudinal study of insulin-like growth factor, insulin-like growth factor binding protein-3, and their polymorphisms: risk of neoplastic progression in Barrett’s esophagus. Cancer Epidemiol Biomarkers Prev, 2007, 16: 2387–95
[66]Gough MD, Ackroyd R, Majeed AW, et al. Prediction of malignant potential in reflux disease: are cytokine polymorphisms important? Am J Gastroenterol, 2005, 100: 1012–18
[67]Kala Z, Dolina J, Marek F, et al. Polymorphisms of glutathione S-transferase M1, T1 and P1 in patients with reflux esophagitis and Barrett’s esophagus. J Hum Genet, 2007, 52: 527–34
[68]Phillips RW, Frierson HF Jr, Moskaluk CA. CDX2 as a marker of epithelial intestinal diff erentiation in the esophagus. Am J Surg Pathol, 2003, 27: 1442–47
[69]Liu T, Zhang X, So CK, et al. Regulation of CDX2 expression by promoter methylation, and effects of CDX2 transfection on morphology and gene expression of human esophageal epithelial cells. Carcinogenesis, 2007, 28: 488–96
[70]Pera M, Pera M, de Bolos C, et al. Duodenal-content reflux into the esophagus leads to expression of Cdx2 and Muc2 in areas of squamous epithelium in rats. J Gastrointest Surg, 2007, 11: 869–74
[71]Sarosi G, Brown G, Jaiswal K, et al. Bone marrow progenitor cells contribute to esophageal regeneration and metaplasia in a rat model of Barrett’s esophagus. Dis Esophagus, 2008, 21: 43–50
[72]Glickman JN, Chen YY, Wang HH, et al. Phenotypic characteristics of a distinctive multilayered epithelium suggests that it is a precursor in the development of Barrett‘s esophagus. Am J Surg Pathol, 2001, 25: 569–78
[73]Hanna S, Rastogi A, Weston AP, et al. Detection of Barrett’s esophagus after endoscopic healing of erosive esophagitis. Am J Gastroenterol, 2006, 101: 1416–20
[74]Hamamoto Y, Endo T, Nosho K, et al. Usefulness of narrow-band imaging endoscopy for diagnosis of Barrett’s esophagus. J Gastroenterol, 2004, 39: 14–20
[75]Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & M criteria. Gastroenterology, 2006, 131: 1392–99
[76]Paull A, Trier JS, Dalton MD, et al. The histologic spectrum of Barrett’s esophagus. N Engl J Med, 1976, 295: 476–80
[77]Harrison R, Perry I, Haddadin W, et al. Detection of intestinal metaplasia in Barrett’s esophagus: an observational comparator study suggests the need for a minimum of eight biopsies. Am J Gastroenterol, 2007, 102: 1154–61
[78]Eloubeidi MA, Provenzale D. Does this patient have Barrett’s esophagus? The utility of predicting Barrett’s esophagus at the index endoscopy. Am J Gastroenterol, 1999, 94: 937–43
[79]Kim SL, Waring JP, Spechler SJ, et al. Diagnostic inconsistencies in Barrett’s esophagus. Department of Veterans Affairs Gastroesophageal Reflux Study Group. Gastroenterology, 1994, 107: 945–49
[80]Montgomery E, Bronner MP, Goldblum JR, et al. Reproducibility of the diagnosis of dysplasia in Barrett esophagus: a reaffirmation. Hum Pathol, 2001, 32: 368–78
[81]Ormsby AH, Petras RE, Henricks WH, et al. Observer variation in the diagnosis of superficial oesophageal adenocarcinoma. Gut, 2002, 51: 671–76
[82]Falk GW, Ours TM, Richter JE. Practice patterns for surveillance of Barrett’s esophagus in the United States. Gastrointest Endosc, 2000, 52: 197–203
[83]Provenzale D, Schmitt C, Wong JB. Barrett’s esophagus: a new look at surveillance based on emerging estimates of cancer risk. Am J Gastroenterol, 1999, 94: 2043–53
[84]Soni A, Sampliner RE, Sonnenberg A. Screening for high-grade dysplasia in gastroesophageal reflux disease: is it cost-effective? Am J Gastroenterol, 2000, 95: 2086–93
[85]Inadomi JM, Sampliner R, Lagergren J, et al. Screening and surveillance for Barrett esophagus in high-risk groups: a cost-utility analysis. Ann Intern Med, 2003, 138: 176–86
[86]Falk GW, Chittajallu R, Goldblum JR, et al. Surveillance of patients with Barrett’s esophagus for dysplasia and cancer with balloon cytology. Gastroenterology, 1997, 112: 1787–97
[87]Jobe BA, Hunter JG, Chang EY, et al. Office-based unsedated small-caliber endoscopy is equivalent to conventional sedated endoscopy in screening and surveillance for Barrett’s esophagus: a randomized and blinded comparison. Am J Gastroenterol, 2006, 101: 2693–703
[88]Lin OS, Schembre DB, Mergener K, et al. Blinded comparison of esophageal capsule endoscopy versus conventional endoscopy for a diagnosis of Barrett‘s esophagus in patients with chronic gastroesophageal reflux. Gastrointest Endosc, 2007, 65: 577–83
[89]Galmiche JP, Sacher-Huvelin S, Coron E, et al. Screening for esophagitis and Barrett’s esophagus with wireless esophageal capsule endoscopy: a multicenter prospective trial in patients with reflux symptoms. Am J Gastroenterol, 2008, 103: 538–45
[90]Gerson L, Lin OS. Cost-benefit analysis of capsule endoscopy compared with standard upper endoscopy for the detection of Barrett’s esophagus. Clin Gastroenterol Hepatol, 2007, 5: 319–25
[91]Rubenstein JH, Inadomi JM, Brill JV, et al. Cost utility of screening for Barrett’s esophagus with esophageal capsule endoscopy versus conventional upper endoscopy. Clin Gastroenterol Hepatol, 2007, 5: 312–18
[92]Canto MI, Setrakian S, Willis J, et al. Methylene blue-directed biopsies improve detection of intestinal metaplasia and dysplasia in Barrett’s esophagus. Gastrointest Endosc, 2000, 51: 560–68
[93]Lim CH, Rotimi O, Dexter SP, et al. Randomized crossover study that used methylene blue or random 4-quadrant biopsy for the diagnosis of dysplasia in Barrett’s esophagus. Gastrointest Endosc, 2006, 64: 195–99
[94]Ragunath K, Krasner N, Raman VS, et al. A randomized, prospective cross-over trial comparing methylene blue-directed biopsy and conventional random biopsy for detecting intestinal metaplasia and dysplasia in Barrett’s esophagus. Endoscopy, 2003, 35: 998–1003
[95]Guelrud M, Herrera I, Essenfeld H, et al. Enhanced magnification endoscopy: a new technique to identify specialized intestinal metaplasia in Barrett’s esophagus. Gastrointest Endosc, 2001, 53: 559–65
[96]Kara MA, Ennahachi M, Fockens P, et al. Detection and classification of the mucosal and vascular patterns (mucosal morphology) in Barrett’s esophagus by using narrow band imaging. Gastrointest Endosc, 2006, 64: 155–66
[97]Sharma P, Bansal A, Mathur S, et al. The utility of a novel narrow band imaging endoscopy system in patients with Barrett’s esophagus. Gastrointest Endosc, 2006, 64: 167–75
[98]Curvers W, Baak L, Kiesslich R, et al. Chromoendoscopy and narrow-band imaging compared with high-resolution magnification endoscopy in Barrett’s esophagus. Gastroenterology, 2008, 134: 670–79
[99]Kara MA, Peters FP, ten Kate FJ, et al. Endoscopic video autofluorescence imaging may improve the detection of early neoplasia in patients with Barrett’s esophagus. Gastrointest Endosc, 2005, 61: 679–85
[100]Poneros JM, Brand S, Bouma BE, et al. Diagnosis of specialized intestinal metaplasia by optical coherence tomography. Gastroenterology, 2001, 120: 7–12
[101]Isenberg G, Sivak MV Jr, Chak A, et al. Accuracy of endoscopic optical coherence tomography in the detection of dysplasia in Barrett’s esophagus: a prospective, double-blinded study. Gastrointest Endosc, 2005, 62: 825–31
[102]Kiesslich R, Gossner L, Goetz M, et al. In vivo histology of Barrett’s esophagus and associated neoplasia by confocal laser endomicroscopy. Clin Gastroenterol Hepatol, 2006, 4: 979–87
[103]Eloubeidi MA, Provenzale D. Health-related quality of life and severity of symptoms in patients with Barrett’s esophagus and gastroesophageal reflux disease patients without Barrett’s esophagus. Am J Gastroenterol, 2000, 95: 1881–87
[104]Shaheen NJ, Green B, Medapalli RK, et al. The perception of cancer risk in patients with prevalent Barrett’s esophagus enrolled in an endoscopic surveillance program. Gastroenterology, 2005, 129: 429–36
[105]Shaheen NJ, Dulai GS, Ascher B, et al. Effect of a new diagnosis of Barrett’s esophagus on insurance status. Am J Gastroenterol, 2005, 100: 577–80
[106]Buttar NS, Wang KK, Sebo TJ, et al. Extent of high-grade dysplasia in Barrett’s esophagus correlates with risk of adenocarcinoma. Gastroenterology, 2001, 120: 1630–39
[107]Reid BJ, Levine DS, Longton G, et al. Predictors of progression to cancer in Barrett’s esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets. Am J Gastroenterol, 2000, 95: 1669–76
[108]Zaninotto G, Parenti AR, Ruol A, et al. Oesophageal resection for high-grade dysplasia in Barrett’s oesophagus. Br J Surg, 2000, 87: 1102–05
[109]Heitmiller RF, Redmond M, Hamilton SR. Barrett’s esophagus with high-grade dysplasia: an indication for prophylactic esophagectomy. Ann Surg, 1996, 224: 66–71.
[110]Konda VJ, Ross AS, Ferguson MK, et al. Is the risk of concomitant invasive esophageal cancer in high-grade dysplasia in Barrett’s esophagus overestimated? Clin Gastroenterol Hepatol, 2008, 6: 159–64
[111]Williams VA, Watson TJ, Herbella FA, et al. Esophagectomy for high grade dysplasia is safe, curative, and results in good alimentary outcome. J Gastrointest Surg, 2007, 11: 1589–97
[112]Peyre CG, DeMeester SR, Rizzetto C, et al. Vagal-sparing esophagectomy: the ideal operation for intramucosal adenocarcinoma and barrett with high-grade dysplasia. Ann Surg, 2007, 246: 665–71
[113]Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med, 2002, 346: 1128–37
[114]Sampliner RE, Hixson LJ, Fennerty MB, et al. Regression of Barrett’s esophagus by laser ablation in an anacid environment. Dig Dis Sci, 1993, 38: 365–68
[115]Berenson MM, Johnson TD, Markowitz NR, et al. Restoration of squamous mucosa after ablation of Barrett’s esophageal epithelium. Gastroenterology, 1993, 104: 1686–91
[116]Sampliner RE, Fennerty B, Garewal HS. Reversal of Barrett’s esophagus with acid suppression and multipolar electrocoagulation: preliminary results. Gastrointest Endosc, 1996, 44: 532–35
[117]Norberto L, Polese L, Angriman I, et al. High-energy laser therapy of Barrett’s esophagus: preliminary results. World J Surg, 2004, 28: 350–54
[118]Ackroyd R, Tam W, Schoeman M, et al. Prospective randomized controlled trial of argon plasma coagulation ablation vs endoscopic surveillance of patients with Barrett’s esophagus after antirefl ux surgery. Gastrointest Endosc, 2004, 59: 1–7
[119]Attwood SE, Lewis CJ, Caplin S, et al. Argon beam plasma coagulation as therapy for high-grade dysplasia in Barrett’s esophagus. Clin Gastroenterol Hepatol, 2003, 1: 258–63
[120]Ackroyd R, Kelty CJ, Brown NJ, et al. Eradication of dysplastic Barrett’s oesophagus using photodynamic therapy: long-term follow-up. Endoscopy, 2003, 35: 496–501
[121]Overholt BF, Panjehpour M, Halberg DL. Photodynamic therapy for Barrett’s esophagus with dysplasia and/or early stage carcinoma: long-term results. Gastrointest Endosc, 2003, 58: 183–88
[122]Johnston MH, Eastone JA, Horwhat JD, et al. Cryoablation of Barrett’s esophagus: a pilot study. Gastrointest Endosc, 2005, 62: 842–48
[123]Sharma VK, Wang KK, Overholt BF, et al. Balloon-based, circumferential, endoscopic radiofrequency ablation of Barrett’s esophagus: 1-year follow-up of 100 patients. Gastrointest Endosc, 2007, 65: 185–95
[124]Fleischer DE, Overholt BF, Sharma VK, et al. Endoscopic ablation of Barrett’s esophagus: a multicenter study with 2.5-year follow-up. Gastrointest Endosc, 2008, 68: 867–76
[125]Ganz RA, Overholt BF, Sharma VK, et al. Circumferential ablation of Barrett’s esophagus that contains high-grade dysplasia: a US multicenter registry. Gastrointest Endosc, 2008, 68: 35–40
[126]Buttar NS, Wang KK, Lutzke LS, et al. Combined endoscopic mucosal resection and photodynamic therapy for esophageal neoplasia within Barrett‘s esophagus. Gastrointest Endosc, 2001, 54: 682–88
[127]Ell C, May A, Gossner L, et al. Endoscopic mucosal resection of early cancer and high-grade dysplasia in Barrett’s esophagus. Gastroenterology, 2000, 118: 670–77
[128]Corley DA, Kerlikowske K, Verma R, et al. Protective association of aspirin/NSAIDs and esophageal cancer: a systematic review and meta-analysis. Gastroenterology, 2003, 124: 47–56
[129]El-Serag HB, Aguirre TV, Davis S, et al. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett’s esophagus. Am J Gastroenterol, 2004, 99: 1877–83
[130]Hillman LC, Chiragakis L, Shadbolt B, et al. Proton pump inhibitor therapy and the development of dysplasia in patients with Barrett’s oesophagus. Med J Aust, 2004, 180: 387–91
[131]Parrilla P, Martinez de Haro LF, Ortiz A, et al. Long-term results of a randomized prospective study comparing medical and surgical treatment of Barrett’s esophagus. Ann Surg, 2003, 237: 291–98
[132]Corey KE, Schmitz SM, Shaheen NJ. Does a surgical antirefl ux procedure decrease the incidence of esophageal adenocarcinoma in Barrett’s esophagus? A meta-analysis. Am J Gastroenterol, 2003, 98: 2390–94
[133]Pohl H, Welch HG. The role of overdiagnosis and reclassification in the marked increase of esophageal adenocarcinoma incidence. J Natl Cancer Inst, 2005, 97: 142–46
[134]Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med, 1999, 340: 825–31
[135]Lao-Sirieix P, Lovat L, Fitzgerald RC. Cyclin A immunocytology as a risk stratification tool for Barrett’s esophagus surveillance. Clin Cancer Res, 2007, 13: 659–65
[136]Keswani RN, Noffsinger A, Waxman I, et al. Clinical use of p53 in Barrett’s esophagus. Cancer Epidemiol Biomarkers Prev, 2006, 15: 1243–49
[137]Scheil-Bertram S, Lorenz D, Ell C, et al. Expression of alpha-methylacyl coenzyme A racemase in the dysplasia carcinoma sequence associated with Barrett’s esophagus. Mod Pathol, 2008, 21: 961–67
[138]Galipeau PC, Li X, Blount PL, et al. NSAIDs modulate CDKN2A, TP53, and DNA content risk for progression to esophageal adenocarcinoma. PLoS Med, 2007, 4: e67
[139]Jankowski J, Barr H. Improving surveillance for Barrett’s oesophagus: AspECT and BOSS trials provide an evidence base. BMJ, 2006, 332: 1512